 Skip to content
Skip to content Sometimes it may be difficult to find love, but certain pathogens, like Helicobacter pylori (H. pylori) are easy to find. This is especially true in the case of Latin America and the Caribbean, which are among the regions with highest rates of H. pylori infection worldwide.
But why should we care?
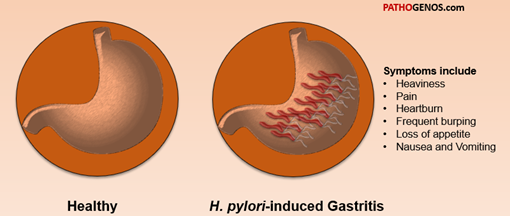
This bacterium, originally referred to as Campylobacter pylori and later reclassified as H. pylori in 1989, is the most frequent cause of mild to chronic gastritis, leading to gastric and duodenal peptic ulcer disease (ca 10-15% of patients), gastric cancer (ca 1% of patients), and gastric mucosa-associated lymphoid tissue lymphoma (MALT) ( See Figure 1).
In 2012, H. pylori infection contributed to 35.4% of new cancer cases associated with infectious pathogens, and for the type of non-cardia gastric adenocarcinoma, the percentage increased to 89%.
Hispanic and Native American /Alaskan Native (NA/AN) patients had the highest prevalence of H. pylori infection associated with upper gastrointestinal (GI) symptoms and diagnosis in a study comparing ethical/racial differences in gastrointestinal symptoms and diagnosis associated with the risk of H. pylori infection in the US.
In a previous blog, I discuss how different Latino cultural background associate with higher frequency of H. pylori infection. In addition, higher percentage of asymptomatic Hispanics had an increased link to H. pylori-associated gastric cancer.
Herein, I discuss some history and overall pathogenesis of H. pylori taking information from the recently published Nature Reviews Disease Primers by Peter Malfertheiner and colleagues.
To note is that scientific review papers are different from peer-reviewed scientific articles. As a review, they summarize the knowledge gathered from published scientific articles in the field.
Discovering the pathogen
The dedicated scientists Professor Warren and Marshal identified H. Pylori as the cause of chronic gastritis in 1982, fulfilling the Koch’s postulates to be classified as a pathogen.
Koch’s postulates were a set of four criteria developed by scientist Robert Koch (1843-1910) to determine whether a microbe can cause disease (i.e., is a pathogen). Emerging pathogens, however, have challenged these postulates as they do not account for pathogens unable to be grown in culture ( e.g., prion diseases).
Before their work, peptic ulcer was once thought to be an acid-driven disease instead of an infection-driven one.
Note. Robert Koch’s postulates developed in the 19th century: (1) the microbe need to only be found in diseased but not healthy people, (2) the microbe needs to be able to be cultured or grown from the diseased person, (3) growing this microbe must lead to the said disease, and (4) the microbe needs to be isolated from the growing medium used to cultivate it and must match the original microbe.
To note is that H. pylori infects half the world population and approximately 80% remain asymptomatic. Despite being asymptomatic, as H. pylori colonies the stomach tissue, it leads to gastritis and/or gastric ulcer with unpredictable and potentially severe outcomes.
Concerningly, although H. pylori is usually treated with antibiotics, many strains of individual isolates of the bacteria are becoming antibiotic resistant.
H. pylori distribution and patterns
Prevalence of H. pylori infection has been linked with multiple factors, including age, ethnicity, geographic regions, socioeconomic status, and hygiene conditions.
Once infected, H. pylori usually remains throughout an individual’s lifetime.
Increased susceptibility to H. pylori varies with genetics and ethnicity, but is also influenced by habits in food sharing, housing habits, and drinking of contaminated water.
Transmission is through direct contact with stool, vomit, or saliva as well as ingestion of contaminated food or water. However, we are still lacking studies on transmission pathways and relative importance.
Transmission between family members especially mothers to siblings is common in developing countries. The extensive food sharing culture of Hispanics could exacerbate this.
Although the paper by Peter Malfertheiner and colleagues mentions how global prevalence of H. pylori has declined due to improved socioeconomic status and hygiene conditions, this is less observed in developing countries, such as Latin America.
H. pylori infection in Latinos
Many scientific studies show how being from a Hispanic/Latino ethnic background increases the chances of H. pylori infection.
For example, by analyzing sera from 284 men in Texas, a study done by Parma et al. show Hispanic men having higher prevalence of H. pylori infection along with higher rates of gastric cancer than non-Hispanic whites. Obesity contributed to this higher prevalence.
Another study published recently in 2022 by Tsang et al., which I previously discussed in detail, emphasizes that H. pylori infection remains a major public health threat in developing countries including Latin America. Their data shows H. pylori seroprevalence remains high and differs significantly by Hispanic/Latino background.
An older paper published in 2014 by Patel et al. showed that H. pylori prevalence was highest in Hispanics (40.9%) followed by Blacks (29.1%) and whites (7.9%).
In tandem, a recent paper published in The LANCET Regional Health by Torres-Roman et al. mention how multiple studies of H. pylori infection in Hispanic/Latino populations in the United States, Latin American, and the Caribbean have shown a sustained prevalence higher than 50% while antibiotic resistance continues to grow.
The nitty gritty of the bacterium
H. pylori is classified as a Gram negative, microaerophilic curved or S-shaped bacteria, with high motility due to their bundle of flagella ( See Figure 3) .
Gram negative means that H. pylori has a thin wall composed of low levels of peptidoglycan (macromolecule consisting of sugars and amino acids) and high lipid content.
This constitution makes H. pylori stain pink or red following the Gram reaction devised by Danish bacteriologist Dr. Hans Christian Gram in 1884 to visualize cocci ( round-shaped bacterium) in lung tissue from patients that had died of pneumonia.
Gram negative bacteria are associated with diseases like meningitis, pneumonia, sepsis, and urinary tract infection. Some Gram negative bacteria include Escherichia coli ( UTIs and food poisoning), Klebsiella ( pneumonia, sepsis), and Pseudomonas aeruginosa. Unfortunately, Gram negative bacteria are typically resistant to antibiotics.
H. pylori contains a small 1.6 Mbp genome consisting of single circular chromosome encoding 1,600 proteins. We can call it small, because In comparison, the human genome is 3.2 billion base pairs long , containing 46 chromosomes (23 pairs) and approximately 80,000 to 400,000 proteins.
The high mutation and recombination rate of H. pylori allows the bacterium to survive in different stomach environment, and it can mutate to adapt to each individual host.
What makes H. pylori so pathogenic?
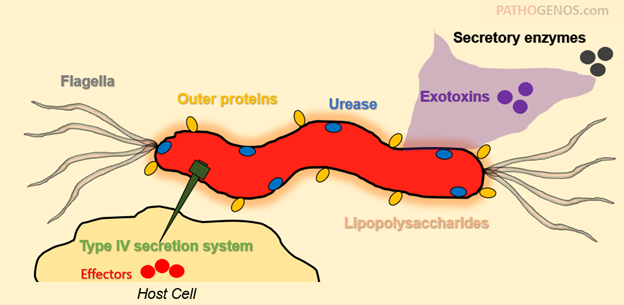
The following include H.pylori’s virulence factors, which are molecules that help the bacterium colonize or take over our body at a cellular level. They allow the bacterium to adhere, evade, and invade cells.
H.pylori likes to move using its flagella
H. pylori moves with flagella driven motility essential for entry of H.pylori into the mucus layer. H.pylori flagella evades toll-like receptor 5 (TLR5) by mutation in an amino acid sequence.
The bacterium direction is controlled by chemotaxis (movement based on chemical stimulus) and energy taxis ( H. pylori monitors its energy levels and swims to a more energy concentrated microenvironment).
The orientation is dependent on pH and bicarbonate along with other constituents in the gastric mucus. To note is that some antibacterial compounds work by inhibiting the motility of H. pylori.
H. pylori uses urease to make itself at home
Urease is essential for H. pylori colonization. It is a high molecular weight metalloenzyme that cleaves urea to ammonia, which is a nitrogen source and elevates the pH in the environment. This enables the bacterium to survive at low pH (i.e., within the gastric lumen) during transmission. Based on knowing this basic mechanism of survival, the rapid urease test was developed to identify bacteria using urease, and it is commonly able to distinguish the genus (taxonomic rank above species and below family) Proteus from enteric bacteria.
Note. An enzyme is a protein that speeds up or catalyzes a chemical reaction. Instead of hours it can now take seconds or minutes to get a product. In this case, produce carbon dioxide which increases the pH, making the solution less acidic. In a way, H. pylori uses Urease to modify its environment so it can thrive
H. pylori hugs gastric cells using its adhesins
Adhesins are proteins in the surface of H. pylori that allow the bacterium to attach to host cell receptors in gastric epithelial cells. This attachment is a crucial step in the initial step in its colonization. H. pylori adhesins recognize specific carbohydrate structures in the surface of host cells. They are a primary target of vaccines against H. pylori infection as they are a key determinant allowing H. pylori to recognize and bind host cells and tissues.
H. pylori uses cagPAI to manipulate host cell machinery
The Cag (cytotoxin-associated gene) pathogenicity island (cagPAI) increases H. pylori virulence helping it colonize the human stomach and induce gastritis, gastric adenocarcinoma, peptic ulcer disease, and atrophic gastritis.
CagA is also the first ever known bacterial onco-protein (protein that induces cellular tumors), which positions H. pylori adenocarcinoma as the second most deadly cancer type worldwide.
CagPAI encodes genes including CagA and components of a type IV secretion system (Cag T4SS).
How it works is that this CagA contains T4SS, which acts as a tunnel to transfer bacterial effector molecules into the cell cytoplasm, like a pirate using a tunnel to get into the ship. These then affect multiple target molecules in the cell thereby controlling cell motility (movement of the cell form one place to another), and inducing reduced cellular tight junctions, genome instability, nucleotide damage, and activation of the Wnt signaling pathway.
H. pylori intoxicates cells by secreting exotoxins
Approximately 50% of H. pylori strains can secrete a powerful tool called vacuolating cytotoxin A (VacA), which is a pore-forming protein. It helps H.pylori channel its way into the cell by forming a anion-selective membrane channels required for its biological activity.
When inside the cells, these toxin prime host cells to begin inducing intracellular vacuoles, apoptotis cell death or necrosis, inducing autophagy, an dinhibiting T cell and B cell proliferation.
In all, because of these toxins, the immune response of the cells are downregulated or decreased and promote H. pylori tolerance.
However, this weapon H.pylori has is not necessary for it to successfully reproduce in the cell. So, it is helpful, but without it the bacterium can continue to “live” and replicate.
Vacuolating cytotoxins are observed in almost all clinical strains of H. pylori but only some strains produce the toxigenic and pathogenic VacA.

